
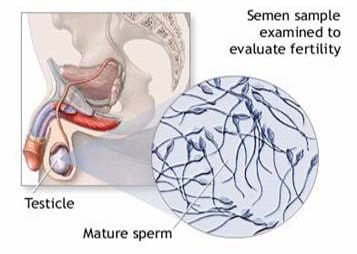
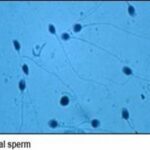
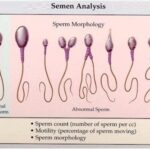
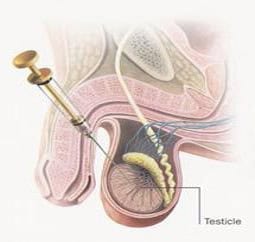
A semen analysis is a male fertility test that assesses the formation and maturity of sperm as well as how the sperm interact with the seminal fluid. A fresh semen sample (no more than a half hour old) is collected and then analyzed in a laboratory for a variety of different factors. In order for sperm to be able to fertilize an egg, it is necessary for seminal fluid to be of the correct consistency as well as for sperm to have maximum motility, ideal morphology, and sperm count. If any of these factors are revealed to be less than perfect in a semen analysis, male fertility may be compromised. Male infertility testing is an important part of making an accurate infertility diagnosis.






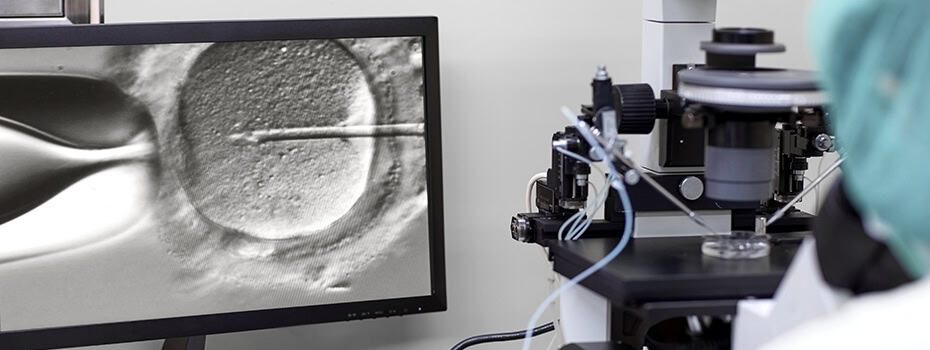
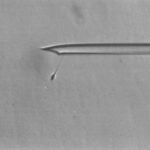
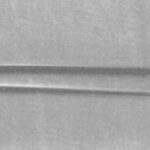
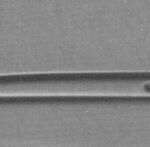
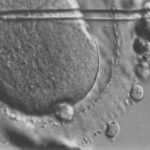
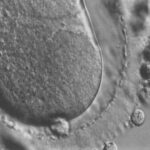
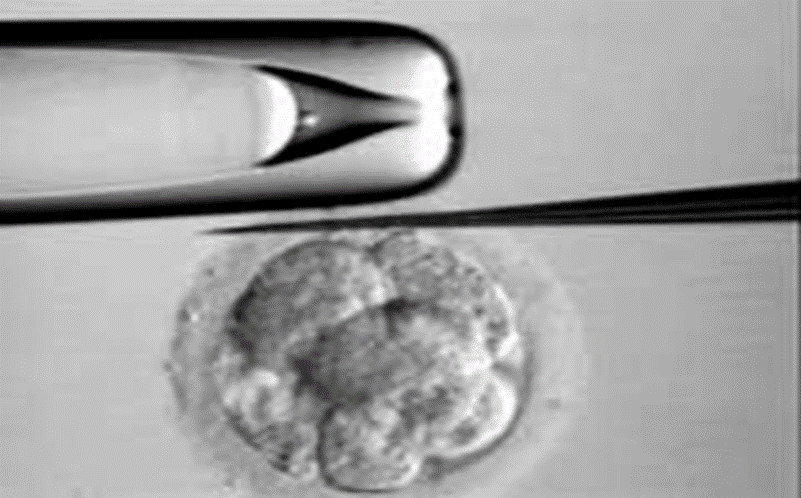
ICSI is a procedure used in conjunction with IVF in which a single sperm is inserted with a micro-needle into the cytoplasm of a mature egg. ICSI is often used if the male partner has very low sperm count, low sperm motility, or poor quality sperm. If fertilization occurs after ICSI, the embryo may then be transferred into the uterus.